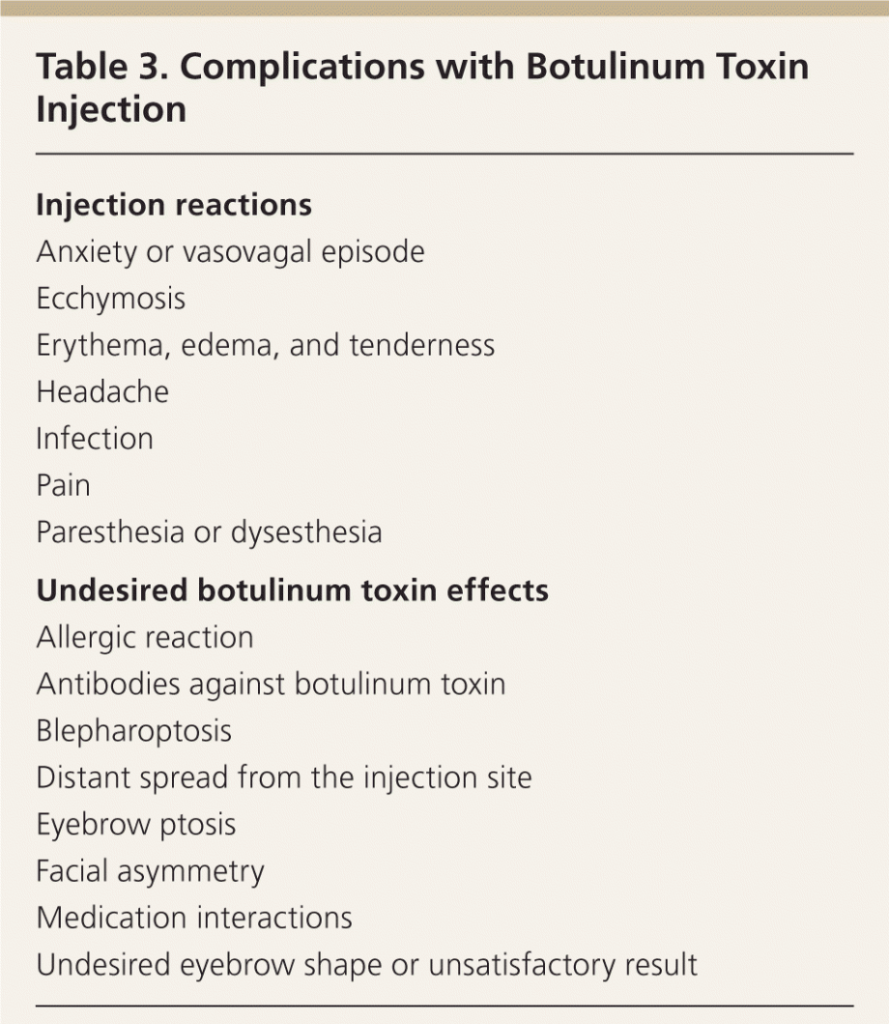
Complications with cosmetic botulinum toxin injections are uncommon and those that occur are usually mild and transient. They can be categorized into injection reactions and undesired botulinum toxin effects.
Injection Reactions
Complications
Complications related to botulinum toxin effects occur less frequently than injection reactions, and are primarily caused by temporary denervation of adjacent muscles outside of the intended treatment area. These complications are technique-dependent; incidence declines as injector skill improves. Temporary blepharoptosis (upper eyelid droop) is uncommon (1% to 5%) but is distressing for patients. It is almost always unilateral, seen as a 2- to 3-mm lowering of the affected eyelid that is most marked at the end of the day with muscle fatigue.
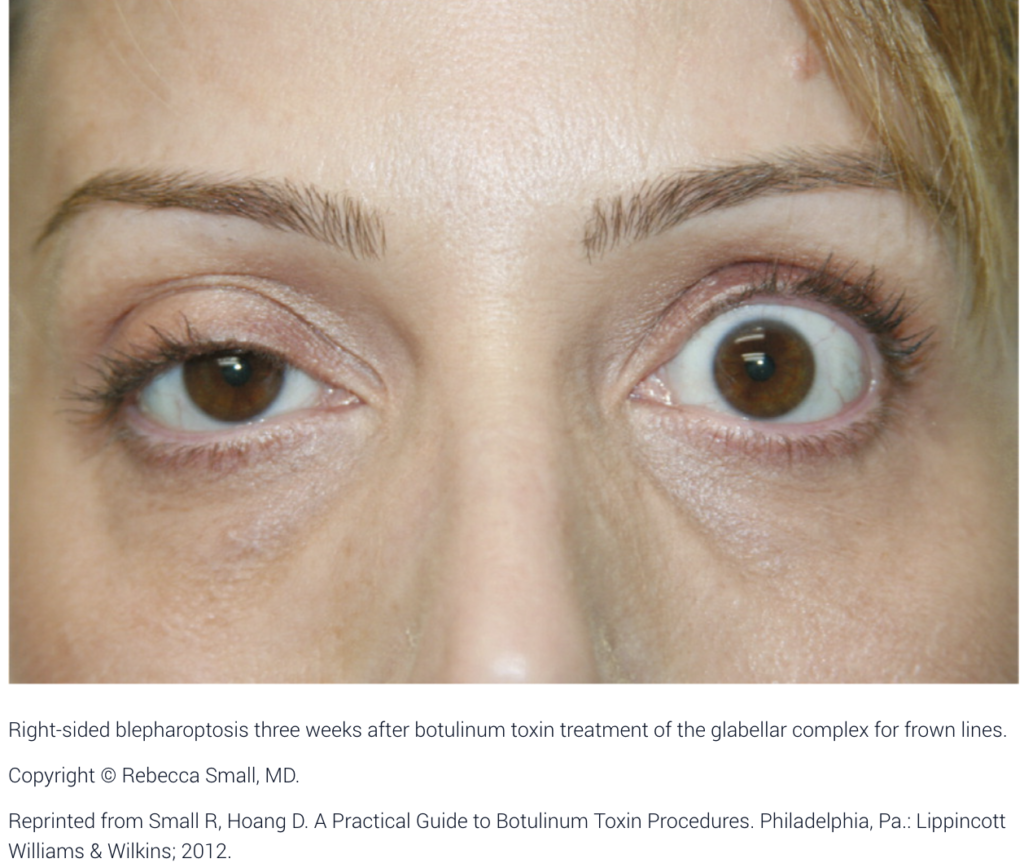
Blepharoptosis is caused by deep migration of botulinum toxin through the orbital septum fascia to the levator palpebrae superioris, an upper eyelid levator muscle. Incidence of blepharoptosis is reduced by placing botulinum toxin injections at least 1 cm above the supraorbital ridge at the midpupillary line when treating the corrugator muscles. Blepharoptosis may be treated using ophthalmic solutions that have alpha-adrenergic effects, such as over-the-counter naphazoline 0.025%/pheniramine 0.3% or prescription apraclonidine 0.5% (Iopidine). Both medications cause contraction of Müller muscle, an adrenergic levator muscle of the upper eyelid, resulting in elevation of the upper eyelid.
Eyebrow ptosis and undesired eyebrow shape are usually related to unintended botulinum toxin effects in the frontalis muscle. Some of these complications can be corrected with botulinum toxin injection in muscles that antagonize the affected muscles; however, complications caused by involvement of adjacent muscles are temporary and will spontaneously resolve as botulinum toxin effects diminish. Facial asymmetry can result from uneven dosing of botulinum toxin. Consistent technique and careful attention to injection volumes at the time of treatment can reduce the incidence of asymmetries.
Citations:
[1] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5300727/
[2] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7874868/
[3] https://pubmed.ncbi.nlm.nih.gov/35178552/
[4] https://pubmed.ncbi.nlm.nih.gov/33128076/
[5] https://my.clevelandclinic.org/health/treatments/8312-botulinum-toxin-injections
[6] https://academic.oup.com/asj/article/42/5/NP327/6530404?login=false
[7] https://emergency.cdc.gov/han/2024/han00507.asp
[8] https://www.plasticsurgery.org/cosmetic-procedures/botulinum-toxin/safety